

































































































































 The Original AMEPilot with Dr. Hanker (still found below) has unfortunately ended. SCAUWG wants to extend a big. "Thank You" to Dr. Hanker for his invaluable contributions to this page.
The Original AMEPilot with Dr. Hanker (still found below) has unfortunately ended. SCAUWG wants to extend a big. "Thank You" to Dr. Hanker for his invaluable contributions to this page.

Going Forward, this page will be devoted to those articles whose topics concern
Medical Information for Pilots.
Preface: (New Content Follows Preface)
Aviation Medical Examiner Information Links:
Guide for Aviation Medical Examiners
Aviation Medical Examiner (AME) portal (GO AME)
AME Seminar Schedule & Registration
AME Online Training Information
Regional Flight Surgeon Contact Info
Medical Certification Information
Sleep Apnea Information:
Let's Begin:
07/24/2026 Aviation medication transparency bill advances - From AOPA - "AOPA-backed legislation 'long overdue' - The Senate Committee on Commerce, Science, and Transportation voted to advance the Aviation Medication Transparency Act (S.3258) on July 22—a bill that would provide needed clarity for pilots on medications they are allowed to take. - The bipartisan bill, which was introduced by Sens. Tammy Duckworth (D-Ill.) and John Hoeven (R-N.D.), would require the FAA to publish—for the first time—a public, user-friendly list of medications that pilots can safely use. The agency would also be required to update it at least once a year. - In a December letter to Duckworth and Hoeven, AOPA endorsed the bill, saying it would provide "long overdue" information that is "critical to pilots." - Duckworth was among the first women in the U.S. Army to..." Continue to Read More.
07/24/2026 Federal Air Surgeon's Medical Bulletin Vol. 60 No. 1 July 2026 - FAA - In this Issue:
- Preflight Your Medical
- Retirement Tribute: Dr. Melchor J. Antuñano Director, Civil Aerospace Medical Institute U.S. Federal Aviation Administration
- The PROTE: Revolutionizing Hypoxia Training
- Your Voice Matters: Participate in the 2026 FAA AME Feedback Survey
- Coming Soon—DMS Updates
- Aviation Medical Examiner Information Links
07/24/2026 Senate Panel Advances Bill Requiring FAA Medication Guidance For Pilots - From AVweb - "A Senate committee advanced legislation that would require the FAA to provide pilots with clearer, updated guidance on medications and medical certification. - A bipartisan bill aimed at giving pilots clearer information about which medications they can take without jeopardizing their medical certification is moving forward in the U.S. Senate. - The Senate Committee on Commerce, Science, and Transportation advanced the Aviation Medication Transparency Act (S. 3258) on July 22. The legislation, introduced by Sens. Tammy Duckworth (D-Ill.) and John Hoeven (R-N.D.), would require the FAA to create and publicly maintain a list of medications that pilots may safely use. The list would also have to be updated at least annually." Continue Here.
07/15/2026 1st LA County case of West Nile virus in 2026 reported in Antelope Valley - From Daily News Health - "Los Angeles County public health officials announced Monday that the first human case of West Nile virus in the county this year involves an Antelope Valley resident who was hospitalized after developing a severe neurological illness. - The patient developed symptoms in late June and was later diagnosed with West Nile virus encephalitis, according to the Los Angeles County Department of Public Health. - “The first human cases of West Nile virus are an important reminder that we all need to take steps to prevent mosquito bites and mosquito breeding,” Los Angeles County Health Officer Dr. Muntu Davis said in a statement. “Mosquitoes thrive in hot weather, increasing the risk of bites and mosquito-borne diseases.”
Davis urged residents to use insect repellent, eliminate standing water around homes where mosquitoes can breed and ensure window and door screens are properly installed and maintained. - Officials also encouraged residents to report neglected swimming pools that could serve as mosquito breeding grounds and to notify authorities when dead birds are found, since increases in infected birds often precede human cases of the virus. - Public health officials said West Nile virus is spread through the bite of an infected mosquito and can cause symptoms including fever, headache, nausea, body aches and skin rash. In severe cases, the virus can affect the nervous system and lead to meningitis, encephalitis, paralysis or death." Continue Here.
07/03/2026 See and Avoid - From AOPA - "The optic nerve is a conduit that transmits visual impulses from the retina to the brain’s visual cortex for interpretation. It contains over a million nerve fibers and is also responsible for eye reflexes, such as pupil dilation, and for maintaining your circadian rhythm. - Pilots are very concerned about hypertension before a flight, during a flight, and before renewing their medical certificate. Our pathophysiology requires regulating many pressures. As pilots, we need to be cognizant of pressure altitude, lift in relation to dynamic pressure, Bernoulli, Newton, Navier-Stokes, and the bending of the wind. Our heart requires a blood pressure of around 130/80 mmHg to perfuse the brain, kidneys, eyes, and peripheral organs. The eyes need to be monitored for high intraocular pressure as we age.
The optic nerve is a conduit that transmits visual impulses from the retina to the brain’s visual cortex for interpretation. It contains over a million nerve fibers and is also responsible for eye reflexes, such as pupil dilation, and for maintaining your circadian rhythm. The optic nerve carries light-dark signals to the brain to help regulate a 24-hour circadian rhythm. The retina converts light into electrical impulses, which travel through the optic nerve to the brain. The brain then converts these impulses into perceptions of color, objects, and spatial depth." Learn More Here.
06/24/2026 Mental Health: All in Our Heads? - From AOPA - "With all the craziness going on in our world now, most of us can probably agree that a form of stress is appreciable in at least some aspects of our head space. - For many, it’s financial issues that just never seem to go away, individual and family health challenges, dealing with the lunacy of bureaucracy and a sense of power from our homeowner’s association president and/or board, the quality of our municipal drinking water, or the fear of shark attacks while ocean swimming.
All completely reasonable concerns. Stress is life and life is stress. We have heard from members over the years who are dealing with the FAA on a mental health issue who assert that flying is what “grounds them” (not in the literal sense!) and helps them think through the circumstances and issues that contribute to their angst and sense of “unwell being.” I’m not saying that’s a good or bad thing, but we all have our built-in coping mechanisms developed over time and experience that hopefully allow us to level the playing field and respond with timely and appropriate actions or thoughts to get us through the crisis." Continue Here.
06/16/2026 National Academies Calls For Crew Radiation Tracking - From AvWeb - "A new report says the FAA has enough science and operational tools in place to begin formal oversight of airline crew exposure. - A new National Academies of Sciences, Engineering, and Medicine report says the FAA should move its established guidance on in-flight radiation exposure into a formal monitoring and management program for Part 121 airline crewmembers. The report, ordered under the FAA Reauthorization Act of 2024, says current science, dose models and operational tools provide a sufficient basis for the agency to begin tracking cumulative exposure while additional research continues.
“Radiation exposure is an unavoidable part of a flight crewmember’s job, and we need to do more to ensure that flight crew health and safety are sufficiently prioritized,” - "The FAA has recognized in-flight radiation exposure for decades and last updated its advisory circular on the subject in 2014. That circular outlines galactic and solar cosmic radiation, recommends exposure limits, gives separate guidance for pregnant crewmembers and directs crews and operators to CARI dose-estimation tools." Find Out More Here.
06/13/2026 Are You Ready for Hypoxia? What Bizav Pilots Need to Know [ From Business Aviation Insider - "Of all the major potential safety threats that aviation navigates, perhaps none can be as stealthy and deadly as hypoxia – a shortage of oxygen in the human body, often resulting in reduced functional ability. - Veteran pilots and industry experts say awareness, planning and training are critical to surviving this life-threatening condition, which can stem from a variety of causes. - Plan to Breathe - In January 2003, the pilot of a Piper PA-28R poorly planned and poorly prepared for a flight from Longmont, CO, to Las Vegas. The unpressurized aircraft without supplemental or portable oxygen flew above 12,500 feet for more than two hours, and..." Continue Here.
credit: AOPA
06/10/2026 The 'Twilight Zone' - Read this letter carefully - From AOPA - "The letter looks like this: “U.S. Department of Transportation, Federal Aviation Administration” in the upper left-hand corner return address, with “AAM–313” hand-stamped underneath it. - This is your letter from the FAA about your airman medical that resulted from it being deferred by your AME, you reporting a new medical problem, or you being the subject of an anonymous tip on the FAA’s tattletale line. You are now in the FAA’s ballpark, also known as the “Twilight Zone.” They make the rules. They are the umpires, and they are the scorekeepers. You must play their game if you want to keep or get your medical. - Do not file this letter away somewhere and hope that it will simply go away. It will not. You must read the letter in detail." - Read about the potential threat to your Medical Here.
06/09/2026 NBAA Champions New FAA Mental Wellness Policy Supporting Counseling - From NBAA - "Washington, DC, June 8, 2026 – The National Business Aviation Association (NBAA) welcomed a recent Federal Aviation Administration (FAA) aeromedical policy update encouraging pilots and air traffic controllers (ATCs) to seek counseling and mental health support early and without fear that receiving talk therapy would jeopardize their medical certification, marking an important shift in the agency’s approach to mental wellness. - Rather than viewing participation in counseling or psychotherapy as a potential red flag, the revised policy explicitly encourages pilots and ATCs to seek help through counseling, psychotherapy and peer-support programs when appropriate. - Further, aviation medical examiners (AMEs) are now directed to..." Continue Here.
06/03/2026 Angel Flight West Fundraiser Tops $1 Million - From AVweb - "The nonprofit said proceeds from the Endeavor Awards will support free medical transportation flights. - Angel Flight West said this week that its 12th annual Endeavor Awards raised more than $1 million in pledges and commitments for free, non-emergency medical transportation. According to the Los Angeles-based nonprofit, the funds will support flight and ground transportation coordination for patients who need care far from home across the western U.S." Continue Here
05/23/2026 Whistleblower Prompts FAA Medical Review Changes - From AVweb - "FAA added medical officers and changed case management procedures after the disclosure.- The U.S. Office of Special Counsel said Thursday it has notified the president and Congress of a whistleblower disclosure involving delays in FAA medical certificate reviews. It said the agency took corrective action but that OSC did not agree with the FAA’s conclusion that the allegations were unsubstantiated. - Post-Issuance Reviews - According to OSC’s May 21 letter, the whistleblower, an FAA medical officer, alleged that understaffing in the FAA Office of Aerospace Medicine delayed the agency’s review of medical certificates that had already been issued by aviation medical examiners. In 2023, AMEs issued 445,613 medical certificates to airline transport pilots, commercial pilots and private pilots, while FAA medical officers were only required to review fewer than 600 of those issued certificates, according to OSC." More Here.
05/16/2026 NTSB Releases Study on Drug Presence Trends Among Fatally Injured Pilots - From NTSB "Potentially impairing drugs found in more than 1 in 4 pilots -
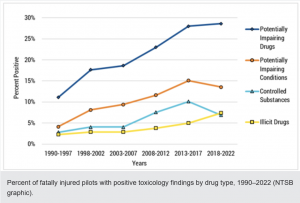
WASHINGTON (May 14, 2026) — The National Transportation Safety Board published a safety research report that found that 52.8% of fatally injured pilots tested positive for at least one drug of any type, and 27.7% tested positive for two or more drugs, continuing an upward trend.
The study examined drug presence identified through toxicology testing of pilots killed in U.S. civil aviation accidents between 2018 and 2022. The report, 2018–2022 Update to Drug Use Trends in Aviation, updates earlier NTSB studies examining drug presence among fatally injured pilots from 1990–2012 and 2013–2017.
Among drug categories identified, the most commonly detected included cardiovascular medications, sedating antihistamines, nonsedating over-the-counter drugs, cholesterol-lowering medications, prostate or erectile dysfunction drugs and illicit drugs.
Detection of potentially impairing drugs increased slightly to 28.6%, with the sedating antihistamine medication diphenhydramine remaining the most detected potentially impairing drug. Illicit drug detection increased to 7.4%, driven primarily by increases in delta-9-tetrahydrocannabinol (delta-9-THC), the primary psychoactive chemical in marijuana.
Researchers also found that drug prevalence varied by pilot age, certification level and type of operation. Drug presence was lower among pilots conducting Part 135 operations than among those operating in general aviation, lower among pilots with an active medical certificate than pilots without an active medical certificate, and lower among pilots holding airline transport and commercial pilot certificates than among pilots holding private, sport or student certificates, or no certificate.
The report emphasizes that the presence of drugs identified through toxicology testing does not necessarily indicate pilot impairment. Instead, the study documents trends in drug detection and provides context for understanding factors that may affect aviation safety.
The safety research report is available on the NTSB website.
To report an incident/accident or if you are a public safety agency, please call 1-844-373-9922 or 202-314-6290 to speak to a Watch Officer at the NTSB Response Operations Center (ROC) in Washington, DC (24/7).
05/12/2026 AOPA Launches Pilot Mental Health Awareness Campaign - From AOPA - "Organization focuses on reducing mental health stigma in aviation. -AOPA is devoting the month of May to pilot mental health, launching a campaign aimed at helping aviators better understand available resources while continuing to push for changes to the FAA medical certification process.
Timed to coincide with Mental Health Awareness Month, the initiative brings together articles, videos, webinars, and interviews centered on a topic that many pilots still hesitate to openly discuss. Concerns over losing a medical certificate have long discouraged some aviators from seeking treatment, even as the FAA has taken steps in recent years to ease pathways for pilots managing certain mental health conditions. - More Info Here.
04/11/2026 BasicMed guidance updated - From AOPA - "AOPA resources overhauled for clarity, ease of use - AOPA has revamped its BasicMed resource page and our online course to make the details more accessible and user-friendly to those aviators who have decided to ditch the traditional FAA medical certificate for a simpler way to maintain their medical eligibility to fly." Read it Here.
02/04/2026 Can You Handle the Pressure, Mr. Woods? - From AOPA - "I laugh out loud every time I watch Mark Gungor’s video “Laugh your way to a better marriage” where he describes the differences between men’s and women’s brains. - He suggests that the male cranium is filled with numerous little boxes, one for the family, one for the car, one for the job, and so on. Importantly, none of these containers touch; quite a clever analogy for how men (in general) think. Recently, a pal was hospitalized with acute compartment syndrome, and little boxes seems like a good place to start.
An airframe is wrapped in skin and has a powerplant, fuel lines providing nourishment, lots of wiring, and rigid bulkheads dividing sections from one another. The human equivalents are the skeleton, skin, muscle, arteries, veins, and nerves, plus a thick, white, fibrous tissue called fascia, and other connective tissues. Pressure plays a role in many areas of aviation; tire pressure, cabin pressure, and manifold pressure. Failing to measure, monitor, and mitigate pressure issues can have serious consequences. Pressure also plays critical roles in humans; obviously blood pressure, but there is also a pressure system inside the head (more of that another day) and pressure inside our limbs. For instance, in the lower leg, the main shin bone—tibia—and adjacent fibula are surrounded by muscle that is nourished by arterial blood, which then drains back to the heart via veins. The entire apparatus is divided into four compartments by fascia." Read more about this Here.
01/18/2026 NBAA Lauds FAA Changes to Medication Requirements - From AINonline - "FAA changes requirements surrounding antidepressants and diabetes - The FAA is continuing to alter its medication requirements to encourage pilots and other aviation personnel to seek mental health care, most recently shortening the wait times for testing on the FAA antidepressant protocol. In addition, it also altered its diabetes management requirements. - Under the former policy, an individual would have to wait six months before..." Find out more Here.
01/16/2026 Title and Subtitle: Operational and Human Factors Considerations for Synthetic Vision Systems and Head-worn Displays: Results from a Literature Review and Survey
The Office of Aerospace Medicine Technical Reports for the U.S. Federal Aviation Administration. This information has recently been updated and is now available. The updated report 26-01 is available in full text.
Authors: Kelene A. Fercho, Bryan L. Watson, Dennis B. Beringer, Theodore C. Mofle, Matthew Scheinblum-Brewer
This research addressed operational considerations from a human factors perspective for the use of synthetic vision systems (SVSs) implemented on a head-worn display (HWD). Given the increasing use and development of SVSs and aviation HWDs, Federal Aviation Administration stakeholders requested information to identify gaps in knowledge to inform future research requirements, and to identify criteria not presently contained in applicable regulations for pilot training and for evaluating equipment functionality, intuitiveness, and potential hazards. This paper includes an overview of commercially available combined vision systems, enhanced vision systems, and SVSs implemented on an HWD; an overview of published scientific literature on SVSs implemented on an HWD; and results from a survey of 70individuals who reported moderate or greater familiarity with SVSs or HWDs. The purpose of the survey was to solicit expert opinion on industry interest, and on human factors and operational considerations of SVSs implemented on an HWD. Example training topics for the use of SVSs implemented on an HWD are included in the Appendix. - No. of Pages: 136
 01/01/2026 Navy Studies Pilot Screening With Virtual Reality - From AVweb - "ASANA project offers data-rich insights into aviator performance. The Naval Aerospace Medical Institute is expanding its approach to pilot candidate evaluation with ASANA, a virtual reality system that tracks cognitive and physiological performance during immersive tasks. Developed by a small team of Aerospace Experimental Psychologists and civilian researchers at Naval Air Station Pensacola, the platform is designed to complement traditional testing methods by capturing subtle indicators of focus, adaptability and spatial awareness. ASANA grew out of the Navy’s long-standing effort to refine the Aviation Selection Test Battery, a process that helps determine who will move forward in flight training for the Navy, Marine Corps and Coast Guard." Read About it Here.
01/01/2026 Navy Studies Pilot Screening With Virtual Reality - From AVweb - "ASANA project offers data-rich insights into aviator performance. The Naval Aerospace Medical Institute is expanding its approach to pilot candidate evaluation with ASANA, a virtual reality system that tracks cognitive and physiological performance during immersive tasks. Developed by a small team of Aerospace Experimental Psychologists and civilian researchers at Naval Air Station Pensacola, the platform is designed to complement traditional testing methods by capturing subtle indicators of focus, adaptability and spatial awareness. ASANA grew out of the Navy’s long-standing effort to refine the Aviation Selection Test Battery, a process that helps determine who will move forward in flight training for the Navy, Marine Corps and Coast Guard." Read About it Here.
12/12/2025 FAA Updates Antidepressant Protocol - From AVweb - "Agency shortens stabilization periods following recent expansion of conditionally acceptable medications. - "The FAA has made a series of updates to its Antidepressant Protocol, including reducing the required stabilization period for pilots and air traffic controllers last week from six months to three. The revision was released Dec. 3 as part of the FAA’s Guide for Aviation Medical Examiners and accompanies broader updates to how antidepressant use is assessed during aeromedical certification. - Those changes in recent months include an expanded list of conditionally acceptable medications, moving beyond SSRIs to incorporate several SNRIs—duloxetine, venlafaxine and desvenlafaxine—along with bupropion and vilazodone. FAA officials have said in recent years that it would make mental health revisions as part of a wider initiative to ensure pilots and controllers have clearer, more efficient pathways for evaluation under the Pilot Mental Fitness framework." Read More Here.
12/11/2025 Adios, off days - From AOPA - "We’ve all experienced off days during our training, when we struggle just to master straight-and-level flight and stay ahead of the airplane. Trying to add new skills doesn’t go well at all. It could be because we are having trouble understanding the new skill we are learning, but it also could be because we are distracted or simply aren’t prepared for the lesson." Read how to better perform Here.
12/01/2025 Development of the FAA Air Traffic Controller Academy Graduate Competency Model - This information has recently been updated and is now available. The updated report 25-55 is available in full text:
Full-Text PDF: Development of the FAA Air Traffic Controller Academy Graduate Competency Model
Authors: L. Cole, E. A. L. LaRose, A. Shiomichi, E. Lentz, J.D. Barrett, C. Sanders
Air Traffic Controller (ATC) training provides new and previous-experience hires the opportunity to learn and practice various knowledge, skills, and abilities (KSAs) required to control air traffic successfully. However, there is a lack of understanding of the minimum competencies and proficiencies new hires possess when they arrive at a field facility, which could influence the field training experience and potentially affect certification rates at the first facility.
To address this gap, a competency model was developed for Tower and En Route training options at the FAA Academy. The Federal Aviation Administration (FAA) Civil Aerospace Medical Institute (CAMI) conducted research directed by the National Airspace System (NAS) Human Factors Research Division, NAS Human Factors Safety Laboratory, AAM-520, to develop a competency model for the expectations for performance of trainees upon successful completion of the Academy training.
In support of this effort, CAMI contracted the services of PDRI by Pearson. The contractor team applied rigorous job analysis methods to develop and validate the competency model. As such, three primary steps were taken: developing a framework and draft competencies and reviewing them with instructors and evaluators, developing and administering a job analysis survey to validate the competencies, and revising the competency model based on the results of the survey. This report provides details on the steps taken to develop the model and present the final model for use within and outside of the FAA. No. of Pages: 57
11/26/2025 Mental Health Reform Bill Sees Senate Introduction - From Plane & Pilot Magazine - "Legislation looks to restructure FAA regulations after passing unanimously in the House. - Senators John Hoeven (R-N.D.) and Tammy Duckworth (D-Ill.) on Thursday introduced to the Senate the Mental Health in Aviation Act aimed at restructuring the regulations governing the FAA’s procedures, encouraging aviation professionals to seek treatment if needed without fear of repercussions." Find Out More Here.
11/12/2025 Medically Speaking: Deep dive into sleep health - From UCLA - Dr. Eve Glazier is exploring the science of sleep health. In the first episode of a two-part series, she talks to UCLA sleep expert Ravi Aysola, MD. They discuss what's happening in your body while you snooze, and four simple rules that can transform your sleep. - Click to Listen on YouTube Here.
11/10/2025 FAA acknowledges BasicMed form error - From AOPA - "To be fixed after shutdown ends - Congress expanded the privileges of pilots flying under BasicMed in 2024, though the new limits are not reflected in the instructions for the Comprehensive Medical Examination Checklist (CMEC), and correcting the form has been delayed by the government shutdown. - The alternative to third class medical certification used by tens of thousands of pilots to medically qualify was expanded by the FAA Reauthorization Act of 2024. As of November 12, 2024, BasicMed pilots have been allowed to fly aircraft weighing up to 12,500 pounds, with as many as seven occupants. FAA Form 8700-2, as the CMEC is otherwise known, however, continues to cite the previous limits (six occupants, 6,000 pounds maximum aircraft weight) on pages 1 and 7. - AOPA flagged the issue to the FAA's attention, and..." Learn More Here.
11/10/2025 The New Blood Pressure Level Experts Recommend to Prevent Dementia - From Money Talks News - STORY & VIDEO - "More aggressive treatment of high blood pressure may be necessary for those hoping to lower their risk of both mild cognitive decline and dementia, according to new expert recommendations. - The American Heart Association and the American College of Cardiology recently issued new guidelines intended to help health care providers both prevent and manage high blood pressure. - This is the first time since 2017 that the guidelines have been updated. Read the Story & View the Video Here.
11/09/2025 A centered ball, and other motion sickness remedies - From AOPA - "During flight training, most of us receive a cursory brief on how to deal with passengers who experience motion sickness but the standard pilot training curriculum offers limited insight about how to prevent it. Several techniques, many of which are foundational to every flight, can help pilots and passengers avoid motion sickness. - The FAA’s Pilot’s Handbook of Aeronautical Knowledge explains that motion sickness “is caused by the brain receiving conflicting messages about the state of the body.” The way we fly can either contribute to or help prevent motion sickness for our passengers. - Try to put your passengers at ease during..." Learn More Here.
11/06/2025 Laughter Is the Best Medicine - From AOPA - Three of my favorite philosophers waxed lyrical about the difference between tragedy and comedy. Aristotle held that tragedies depict people who are better than we are, while comedies represent people who are worse. - Charlie Chaplin reportedly said: “The difference between tragedy and comedy is distance. Up close, things seem tragic. Distance yourself from it, and you get comedy.” And Mel Brooks nailed it: “Tragedy is when I cut my finger. Comedy is when you fall into an open sewer and die!” We inherently know that negative emotions bring with them unpleasant somatic symptoms, and laughing feels good, but is it actually good for you? - Well, here is the headline: yes, laughter is, if not the best, then at the least, very good medicine. Aviators live by checklists that guide us through processes to keep us safe. But adding laughter to the POH can improve your health and safety, and not just in the cockpit. Compelling data demonstrates that..." Read More Here!
10/29/2025 A Stroke of Fate - FAA - "There are distinct differences between a BasicMed “qualification” and an FAA-issued medical “certification.” - FAR 61.53 governs all piloting operations and requires that we medically “self-assess” that we are fit and safe to fly during the time that either a medical certificate or BasicMed qualification is in effect. However, there are several “off-ramps” for self-certification that require a detour in the way of a special issuance medical before exercising BasicMed privileges.
There are eleven specific medical conditions, taken directly from the Part 67 medical standards, that require a one-time special issuance before you can start or continue with BasicMed. One of those is a “transient loss of control of nervous system function(s) without satisfactory medical explanation of the cause.” This is one of the “closet catch-all” regulations that needs a bit of a deep dive to fully understand. - Cerebrovascular disease, a common accomplice of “heart disease,” or atherosclerosis, is the result of a buildup of arterial “plaque” that forms over time in the arterial blood supply. These nasty fatty deposits are made up of..." Continue Here.
0/04/2025 Pilots Gain Greater Flexibility, Faster Recertification in New FAA Medical Guidance Update - From NBAA - "The FAA recently released significant updates to its medical guidance for aviation medical examiners (AME Guide) that considerably reduce required no-fly limits for key medical conditions and surgeries, making it easier for pilots to maintain their medical certifications. - One of the most notable changes is a reduction in the required observation period for cataract surgery. Previously, pilots had to wait up to two years before medical recertification was allowed, but under the new rules, this wait time has been reduced to just three months." Continue Here.
0/04/2025 Mitigate Inflight Medical Emergencies With a Proactive Approach -From Business Aviation Insider - "Most pilots are formally trained for every type of routine and emergency situation. But an inflight medical emergency is usually not among them. - There currently are no federal requirements for any emergency medical training. After all, the chance of a passenger suffering a serious medical problem is minimal. - “From the studies we’ve done, there is a 1-in-604 chance that a commercial flight will have an inflight medical event,” explained Dr. TJ Doyle, M.D., MPH, medical director, communications and aviation consultation at University of Pittsburgh Medical Center/STAT-MD Services. “On the business aviation side, the frequency is orders of magnitude smaller, simply because the passenger count is so much lower.” -
“The most common are syncopal events, which are those where someone feels like they are going to pass out,” he said. “There’s also a condition called vasodilation [dilation of blood vessels] where someone’s blood pressure goes down quickly, causing light-headedness or fainting.” - Learn More About What Might be Beneficial Here.
09/17/2025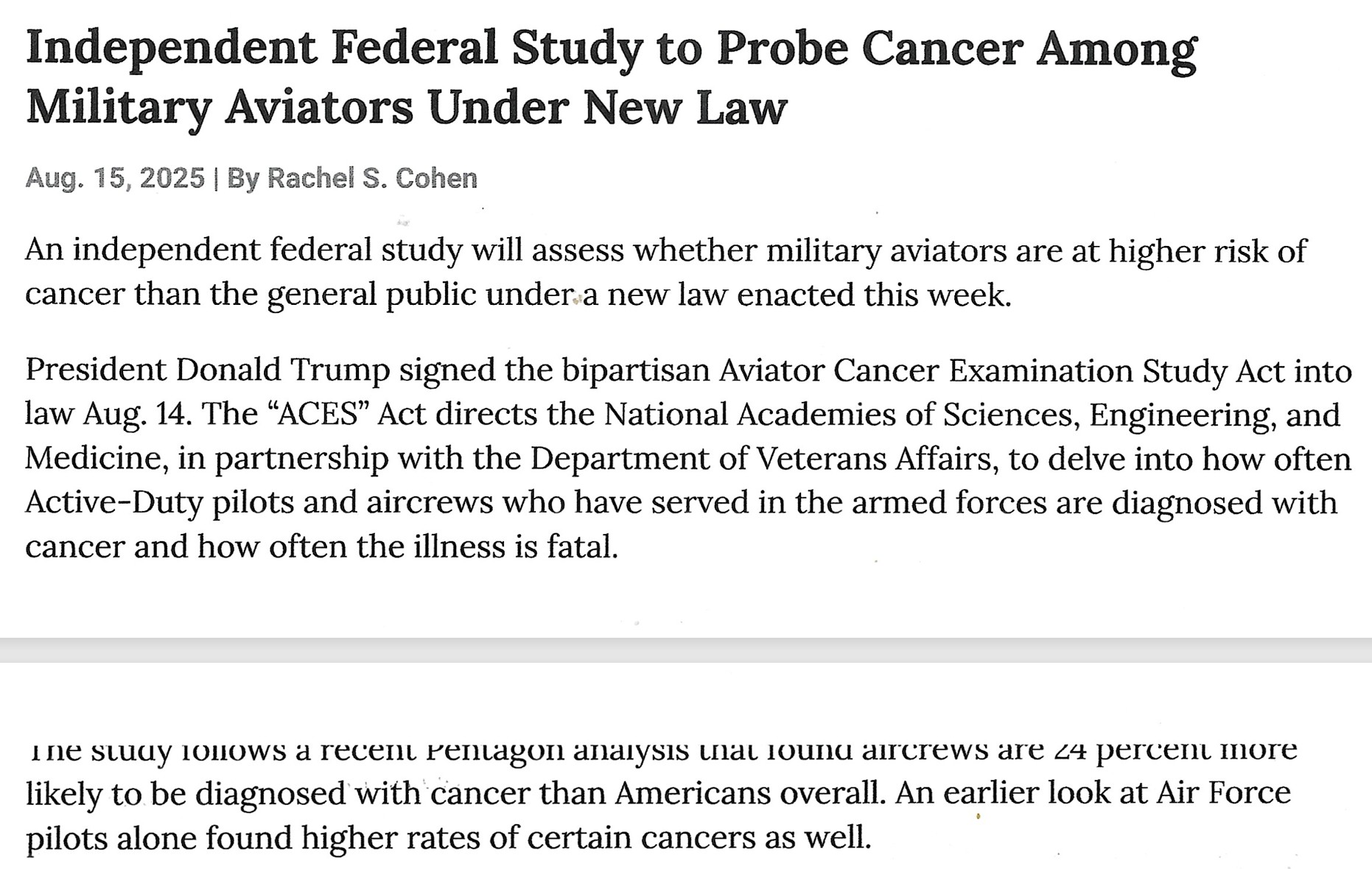
A Fascinating Informative Article from Air & Space Forces Magazine. Finish Reading Here.
09/14/2025 Mental Health in Aviation Act Moves to Senate - From AVweb - "Bill aims to reduce barriers to help and modernize FAA regulations around mental health in aviation. - The U.S. House of Representatives passed the Mental Health in Aviation Act of 2025 on September 9. First introduced by Representatives Sean Casten of Illinois and Pete Stauber of Minnesota, the legislation would require the FAA to revise medical certification regulations in order to help pilots and air traffic controllers seek treatment and voluntarily disclose mental health conditions with fewer professional barriers or potential implications.
The act calls for the FAA to consult with aviation labor groups, medical examiners, and other stakeholders while drafting new rules. It also directs the agency to conduct annual reviews of its mental health special issuance process, reclassify and approve additional medications, and expand examiner training." Read About It Here.
08/30/2025 VA disability and FAA medicals - From AOPA - "The past few years have been tumultuous for pilots receiving medical disability benefits from the Department of Veterans Affairs." Continue
08/23/2025 Generative AI Powers Parkinson’s Drug Development - From AI*Business - Insilico Medicine said its novel medication could be a “paradigm shift” in Parkinson’s treatment - A biotech company using generative AI for drug development has announced a new “potentially transformative” therapy for Parkinson’s disease. - Insilico Medicine said the orally available drug, ISM8969, was developed using its proprietary Pharma.AI platform. The generative AI-powered solution is used for the design of novel molecules with potential applications across biology, chemistry, medicine development and science research. - ISM8969 completed initial studies with favorable results. Assessed across three motor capability tests, the drug was shown to improve motor abilities in mice treated with the medication." Continue Here.
08/23/2025 NASA, Google Testing AI for Medical Care in Space - From AI * Business - "The new tool could help astronauts diagnose and treat medical issues without real-time contact with Earth - Google and NASA have announced a new partnership to bring AI-enabled medical care to spaceflights. - The news comes as NASA prepares for its new Artemis mission to return to the Moon, with investigations underway into how to conduct remote diagnoses and treatments to crew without a physician or when real-time communication with Earth may not be possible. - “Supporting crew health through space-based medical care is becoming increasingly important as NASA missions venture deeper into space,” the partners said in a statement." Continue Here.
8/23/2025 Exploring the Relationship between Operational Errors and Color Vision Deficiency
Authors: Crutchfield, Jerry
We analyzed Operational Error (OE) data and data from the Office of Aerospace Medicine that identified 87 Color Vision Deficient (CVD) Air Traffic Control Specialists (ATCSs) to explore the relationship of color vision deficiency with the occurrence of OEs. Our first analysis searched 70 OE narratives, recorded across 12 years, for OEs where CVD ATCSs were involved. We found no reports that identified color vision or the inability to distinguish colors as a possible contributor to a loss of separation. Next, we attempted to determine if CVD ATCSs were involved in a similar number of OEs as their Color Vision Normal (CN) co-workers. We compared number of OEs occurring from 1995 to 2006 for 87 ATCSs identified as CVD with two sets of matched pairs of CN ATCSs to determine if CVD ATCSs were at a greater risk of being involved in an OE as compared to CN ATCS. We matched CVD ATCSs with CN ATCSs who had the same number of years of experience, worked in the same type of facilities, and were approximately the same age. The comparison of the number of OEs between the three groups was inconclusive due to the small effect size associated with the occurrence of OEs and the resulting lack of statistical power. However, a significant difference was found between the number of OEs in which CVD ATCSs were implicated during the time period from 2001 to 2006 as compared with the time period from 1995 to 2000. The number of OEs in which CVD ATCSs were involved went up after the introduction of ATC display systems in the year 2000 that made more use of color. No. of Pages: 26
07/20/2025 The science of aging - From AOPA - "The Secret Antidote to Growing Old - "A while back one of the posts was on “The Fountain of Youth“ where I talked about new meds that slowed down some of the ill effects of getting older. We also talked about other factors in our environment and diet that accelerated aging in the post on “We’re Not Aging Well.” That, and the stuff about THC, was all about the symptoms of getting old; there wasn’t anything there about the basic process and science of aging, so let’s get to it. - There are three ways we think about aging. The first is appearance, and in these days of social media “influencers” that one gets the most attention, even though it’s the least important of the three." Full Article Here.
07/18/2025 Pilot Incapacitation Suspected In California Incident - From AVweb - "Cessna Corvalis single dropped off of radar about 2.5 hours after overflying its destination airport. - An incident over the weekend is raising concerns over the problem of pilot incapacitation. On Sunday afternoon, Cessna T240 Corvalis TTx (N636CS) departed from Ramona Airport (KRNM) in California for a short flight to Montgomery-Gibbs Executive Airport (KMYF) in San Diego. While about 8 miles from the destination airport, the pilot accepted a clearance to intercept the final approach course for Runway 28R. It was the last communication received from N636CS." Continue.
 07/14/2025 Mayo Clinic Concept: Remote Flight Physicals - From Aviation Consumer - "As the field of AMEs continues to thin and demand for FAA medical certification rises, kiosk-based flight physicals could make a lot of sense. -
07/14/2025 Mayo Clinic Concept: Remote Flight Physicals - From Aviation Consumer - "As the field of AMEs continues to thin and demand for FAA medical certification rises, kiosk-based flight physicals could make a lot of sense. -
he respected Mayo Clinic’s Aerospace Medicine department seems the perfect clinical advisor to the FAA, particularly at a time when the agency’s medical certification division can’t seem to keep up with demand.
Moreover, with large health care companies buying up mom-and-pop medical practices, there’s a huge shortage of AMEs available to administer exams and issue medical certificates. That’s grounding otherwise capable and fit pilots. With virtual medical visits common in the pedestrian world, why not virtual visits with AMEs, too? - Through biometric software embedded in exam kiosks, the Clinic is working on a proof of concept to show that it is possible for a pilot to use an app to set up a visit and coordinate with a remote examiner. Still in a pretty rudimentary stage, the Clinic has simulated roughly 20 pilots through the kiosk concept." Finish Reading Here.
07/11/3025 Court Orders FAA To Explain Mental Health Drug Denial - From AVweb - "Judges want to know why some effective antidepressants can't be used by pilots. - The FAA has to give better reasons for denying a former airline pilot a medical for taking an unapproved anti-depressant drug. In a decision released June 27 by three judges of the U.S. Court of Appeals for the District of Columbia Circuit’s, the agency was told to provide more solid rationale for its categorical ban on the drug mirtazapine. Michael Solondz was put on Lexapro for anxiety in 2018 after going through a rough patch with the death of his father. That drug is on the FAA’s list of conditionally approved anti-depressants, but it caused unwanted side effects for Solondz. His doctor switched him to mirtazapine and it effectively treated the anxiety without the side effects. But mirtazapine is not on the FAA’s list of conditionally approved antidepressants and it has blocked Solondz from restoring his medical. The judges stopped short of telling the FAA to approve the medical but they want a better explanation of why the drug that doesn’t work for Solondz is approved and the one that does work for him can’t be. - The judges noted that even if Lexapro worked for Solondz, there was no guarantee he..." Continue Here.
06/21/2025 FAA updates MedXPress to speed up medical certification - From AOPA - "The FAA has updated the MedXPress system to streamline the medical certification process, the first of “many steps” the agency plans to take to make it “clearer and faster. - Changes stem from AOPA, industry feedback - The updated MedXPress landing page now features (under the “Help” tab) links to resources such as system guides, an FAQ, an aviation medical examiner (AME) locator, and the FAA’s online Guide for Aviation Medical Examiners. - The goal is to help applicants better prepare their medical submissions before visiting an AME, reducing the need for time-consuming requests for additional information. - Among the updates are new on-screen prompts that encourage applicants to review requirements for any known medical conditions in advance. First-time users are also provided with...
" Read More Here.
06/18/2025 Mayo Clinic Concept: Remote Flight Physicals - As the field of AMEs continues to thin and demand for FAA medical certification rises, kiosk-based flight physicals could make a lot of sense. - From Aviation Consumer - "Mayo Clinic has played an important role in aviation medical certification since 1920, when several of the Clinic’s docs served as the first pilot medical examiners for the Civil Aeronautics Board, the precursor to the FAA. Contributions include developing the first high-altitude pressure chamber in North America, a simulator for training World War II pilots, plus the BLB supplemental oxygen mask and the A-14 mask and bailout bottle. It’s a rich heritage and while there is a lot more aeromedical research needed, the 2021 pandemic put a lot of studies on hold because pilots couldn’t come to the Clinic. That turned out to be a unique opportunity that leads to the question of whether in-person FAA medical exams are even necessary. - Today a large focus of the Mayo Clinic’s Aerospace Medicine division (in conjunction with the FAA) is developing a plan for ..." Continue Here.
05/24/2025 InFO 25005, Transportation of Human Organs in the Cabin of an Aircraft used in Title 14 Code of the Federal Regulations (14 CFR) Part 121 Operations, has been published. - This InFO provides information to air carriers conducting part 121 operations on the transport of human organs in the cabin of an aircraft - The InFO can be viewed by downloading the attached .pdf files or by clicking on the following link,
https://www.faa.gov/other_visit/aviation_industry/airline_operators/airline_safety/info/all_infos/
05/11/2025 Understanding Seizures - From AOPA - "As an adjective, fit implies good general health, meeting the requirements to pilot an aircraft, and clothing that is size-appropriate. - Epilepsy is derived from Greek epilambanein, meaning to seize or attack because the person involved may be overwhelmed when it happens. Seizures occur when there are brief episodes of..." Get the data you need, Click or Tap: Understanding seizures
05/11/2025 Historic FAA Decision: Pilot with Active ICD Granted Special Issuance Medical Certificate - From AOPA - "Barnett Law Offices recently represented a Delta Air Lines pilot who suffered a cardiac arrest while operating a 777 from Frankfurt, Germany, to Chicago in May of 2020. - The captain was able to resuscitate the pilot, a first officer, after using CPR and the on-board emergency defibrillator. The flight diverted to Canada because of the emergency created by the pilot’s cardiac arrest. The pilot was initially treated in Canada and received an active ICD, which allows for continuous monitoring of his heart function, and, if needed, can deliver an electronic shock to bring the heart back into rhythm." Full Article Here.
05/11/2025 Title and Subtitle: Spatial Disorientation in Fatal General Aviation Accidents (2003 – 2021) - FAA - "The incidence of spatial disorientation (SD) during flight poses a distinct threat in general aviation (GA) due to the high fatality risk associated with its occurrence. While historical analyses have examined the incidence of SD in GA accidents, little current research exists. This research examines fatal GA accidents associated with SD from 2003 to 2021 and investigates the pilot demographics, flight characteristics, and environment conditions associated with these accidents to identify potential risk factors and compares these findings with previous historical analyses." Full-Text PDF:Spatial Disorientation in Fatal General Aviation Accidents (2003 – 2021)
04/28/2025 FAA Seeks Input on Improving Medical Process - Thursday, April 24, 2025
WASHINGTON — The FAA will immediately begin evaluating suggestions that aviation stakeholders offered during a listening session Wednesday about improving the airman medical process.
“I like to talk about safety being a team sport and certainly this is part of that process to make things better,” Acting FAA Administrator Chris Rocheleau said in his opening remarks. “Clearly there are things that are not working for everyone.”
Rocheleau also delivered some welcome news: the FAA will not proceed with a plan to issue initial denials to pilots who provide incomplete examinations or paperwork.
“There was a lot of [stakeholder] feedback, and we took it seriously and we are not going to do that,” he said.
FAA Federal Air Surgeon Dr. Susan Northrup began the session by explaining the challenges the agency faces in evaluating medical certificate applications and initiatives it’s pursuing to speed up the process.
Challenges include record high applications, which reached about 450,000 in 2024 compared to a recent annual average of about 385,000; a doubling of Special Issuance medical certificates since 2019, which take more work to process; and incomplete information on airmen’s submissions.
FAA initiatives include improving the online MedXPress portal and FAA-industry working groups tasked with modernizing the medical process including continuing the work of an earlier mental health rulemaking committee.
One clear message from stakeholder participants was that they’re eager to help explain how the FAA has improved the process so far, to dispel misconceptions about timelines. The groups also collaboratively developed a checklist on how to prepare for a medical exam, which they will begin distributing to their members.
They offered a host of creative ideas for improving the process, including:
- Create a plain-language version of the Guide for Aviation Medical Examiners so pilots can better understand requirements.
- Clarify confusing questions on medical certificate application forms.
- Encourage pilots to report medical conditions by providing information about how long it takes to resolve common issues.
- Identify the top five diagnoses by age group and provide information on how to address them, using flow charts or checklists.
- Create a webpage with QR codes that lead to information on common conditions.
- Recruit pilots to do video testimonials about how their conditions were resolved.
Participants included representatives from the Air Line Pilots Association, Aircraft Owners and Pilots Association, Allied Pilots Association, Coalition of Airline Pilots Associations, Experimental Aircraft Association, Independent Pilots Association, National Association of Flight Instructors, National Business Aviation Association, National Flight Training Alliance, Southwest Airlines Pilots Association, and Vertical Aviation International.
04/26/2025 FAA withdraws medical denial policy proposal - From AOPA - "Instead, FAA partners with AOPA, industry on pilot medical education campaign - The FAA announced during a meeting with aviation industry organizations on April 23 that it will not implement its proposed policy that would have replaced the longstanding practice of deferring incomplete medical applications with issuing immediate denials." Continue Here.
- Over-the-counter medications
- Prescription medications in gel, liquid or aerosol form
- Ice packs or gel packs for medically necessary items
- Food and drink for infants and toddlers
- Wet batteries
- Live fish transported in water
- Biological specimens
- Breast milk or baby formula
- Liquid-filled teethers
- Duty-free items sealed in a tamper-evident bag
- Fresh eggs
However, bear in mind that not every airport has adopted this rule yet, so it's crucial to check each airport's rules on their website before you depart.
04/07/2025 More Smoke - "Last month I used this space to talk about the risks from vaping and cigarette smoke. Recent events in California with the tragic out-of-control wildfires call for a more detailed look at the health risks of smoke from other sources that also get into our lungs. For me it’s a very personal issue, having moved here to the southeast from Southern California.- The air pollution from smoke and airborne particles generated by the fires is a toxic cauldron of petrochemicals, ozone, nitrogen dioxide, sulfur dioxide, and carbon monoxide. When wildfires burn up whole communities, particulate matter from chemicals, plastics, insulation, construction materials, and home furnishings is scattered into the air. This particulate matter carried in the wind poses a real public health threat from both short- and long-term exposures. While particles from wildfire smoke vary in size, about 90% of the particle mass emitted consists of fine granules that are about the size of a single human hair. These little beasts are coated with all sorts of noxious junk including acids (specifically sulfuric acid), inorganic compounds like ammonium sulfate, ammonium nitrate, sodium chloride, petrochemicals, organic chemicals, soot, metals, soil or dust particles, and biological materials such as pollen and mold spores. - Find out more of the ways you can be affected Here.
04/07/2025 Operational Human Factors Considerations for Head-Worn Display (HWD) Usage in Civil Aviation
Full-Text PDF: Operational Human Factors Considerations for Head-Worn Display (HWD) Usage in Civil Aviation
Authors: Susindar, S., Ferris, T., Valasek, J., Fojtik, E., Brown, M., Pugh, K., Marcario, C., and King, T.
"Advanced visual display systems, such as Head-Up Displays (HUDs), Helmet-Mounted Displays (HMDs), and Head-Worn Displays (HWDs), have been used in military aviation since the 1960s and have been increasingly introduced in general and commercial aviation cockpits. The evolution of in-cockpit technology has ushered in fundamental changes in how pilots receive and process flight-relevant information. Flight operations proceed very differently in cockpits outfitted with traditional head-down display (HDD) configurations compared to those that support viewing/interacting with HUDs, HWDs, and other types of advanced visual displays. The physical and cognitive demands placed on pilots are also impacted by the use of these technologies. Therefore, it is important to understand the nature of these interactions, the demands imposed, and the implications of display system features for safe and effective aviation, communication, and navigation. This report details a hybrid narrative and systematic literature review of human factors issues related to aviation applications of HWDs and other advanced visual displays. It summarizes the scientific findings of studies on HWD usage and compiles evidence that can inform recommendations for the usage of HWDs in civil aviation." No. of Pages: 101
04/05/2025 Flight Rules Change For Pregnant Military Pilots - "Pregnant U.S. military pilots can fly to 32 weeks after taking the first three months off. - Pregnant military pilots have had their wings clipped but also received an extension in their flying window under new rules announced by the Pentagon. The military says flying will be banned during the first trimester, when the chance of miscarriage is greatest, but after the first 13 weeks they can actually keep flying for longer, up to the 32nd week instead of 28 weeks. Flying anything with an ejection seat is banned for the full term of the pregnancy. - To fly while pregnant, military pilots have to apply for a medical waiver, and..." Finish reading Here.
03/17/2025 Guest Blog: FAA Quietly Adds Special Issuance Medical Expiry Dates - "Some special issuances come with an end date that other medicals don’t have. - Sometimes, medical certificate applicants find themselves outside the "four corners" of Part 67. Such persons can still apply for (and be issued) medical certificates under the discretionary issuance Section 67.401. However, such persons are typically then subjected to an alternative set of eligibility requirements that exist only in a policy document called the Guide for Aviation Medical Examiners ("GAME"). While the GAME is publicly available, it is directed at AAM designees, and AAM changes it regularly without advance notice to the public. - AAM has begun in the last few years to sometimes impose a “drop-dead” date in the Limitations section of some "special issuance" medical certificates." Find out more Here.
03/16/2025 Counterfeit Medicines - "Heard the one about the chap claiming to be a professional counterfeiter? He had the documents to prove it! Counterfeit derives from Old French—contre (“counter or against”) and faire (“to make”), the combined meaning “to make an imitation.” - "In the example above I reference statins; buying online might bypass the doctor asking key questions that could mitigate medical risk. Another example is purchasing drugs to treat erectile dysfunction (https://pilot-protection-services.aopa.org/news/2022/april/01/dont-come-crying-to-me-when-youre-the-lonely-one), which has many causes, including emotional stressors, low testosterone and serious cardiovascular disease. Men who develop ED should see their doctor and not just buy a solution online; it is dangerous!" - Read the FULL STORY Here - It is Important.
03/16/2025 Cherokee County man cured of sickle cell anemia complications at Atlanta hospital, he says - "Kyle Registre has known since he was a child that he wanted to become a pilot. But, as he got older, he realized having sickle cell disease would make flying a challenge. VIDEO - "Georgia man pursues pilot license despite sickle cell" - Story and Video Here.
03/16/2025 No rewards for fighting fatigue - "When I began my flying career, it was common for pilots to be derided for calling in sick or fatigued. In fact, management often made enough of a hassle for calling in fatigued that most pilots just called in sick. - The problem with this approach is that it obscured too many potential data points that could have furthered the understanding of fatigue and its causes. - Airlines were required to train pilots on fatigue, its causes, and appropriate remedies. The term “strategic use of caffeine” was one that I always felt was insulting. I don’t drink coffee, and I drink caffeinated soda only a handful of times a year. Telling us to avoid caffeine while also telling us to use it strategically sounded to me like the ultimate “wink-wink” scenario: Fatigue is for the weak, so do what you must to complete the mission.
While we all knew that fatigue existed, it was often either ignored, or was simply not discussed. Fortunately, science and common sense have made progress. Unfortunately, that progress has been stained with blood, as several accidents have driven home the importance of understanding fatigue. Colgan Air Flight 3407 is the best-known example, but not the only one." Read More from the AOPA article Here.
03/16/2025 Industry Attitudes About Pilot Mental Wellness May Be Shifting - From Business Aviation Advisor - "The aviation community, including the FAA, has been showing signs of progress regarding pilots who are seeking support and treatment for mental health issues. - Industry recommendations addressing mental wellness concerns among pilots, and revised FAA guidance to aviation medical examiners (AMEs), mark progress toward not only the proper treatment of mental health, but also greater understanding of these issues across the industry, including in business aviation.
The Mental Health & Aviation Medical Clearances Aviation Rulemaking Committee (ARC) published a comprehensive list of recommendations to the FAA last year addressing concerns about mental health from across the aviation community. - Formed in late 2023, the ARC was tasked with five primary responsibilities. Topping that list was identifying factors that discourage those in the aviation industry from disclosing mental health concerns, including stigmatization and fear over the potential loss of a pilot’s medical certification. - “One key recommendation was..." Continue reading about Pilot Wellness Here.
Epilepsy is derived from Greek epilambanein, meaning to seize or attack because the person involved may be overwhelmed when it happens. Seizures occur when there are brief episodes of abnormal electrical activity generalized across the entire brain or very focal. If the latter, the symptoms experienced are predictable based on which part of the brain is firing randomly. They can result from many causes, including bacterial, viral, or other infectious diseases causing swelling of the brain or its surrounding membranes, the meninges (hence meningitis) and high fevers from other infections, especially in children.
Trauma can also induce..." Continue Reading Jonathan Sackler's article Here.
03/10/2025 Best Of The Web: Pilot Wages Public Fight To Get Her Medical Back - VIDEO - "Xyla Foxlin had her medical pulled for a common condition related to her choice of birth control. She’s fighting it. - When Xyla Foxlin visited her gynecologist for the routine replacement of her IUD it set off a chain of events that ultimately led to her being found medically unfit to continue flying her beloved Cessna 140. She's harnessing her considerable talent as a social media influencer and YouTuber to draw attention to the plight of thousands of pilots with treatable or even curable mental health issues who dare not be honest about their conditions for fear that what's happened to her might happen to them. She's part of a group trying to get Congress to support the Mental Health In Aviation Act." Continue Here.
03/04/2025 FAA Paperwork Medical Denials Delayed ‘Indefinitely’ - "Policy would have turned medical deferrals into denials if paperwork wasn’t complete.- Sources have told AVweb that a controversial FAA policy to turn incompletely documented medical deferrals into denials has been indefinitely deferred. The policy was supposed to have come into effect on Jan.1, but opposition from a broad base of GA groups prompted a deferral until March 1. The indefinite delay was communicated to AMEs on Monday. - The policy would have seen anyone whose medical was deferred by..." Continue Here.
02/05/2025 It's Not All Honey - "Dr. Kenneth Stahl explores the negative--and surprisingly positive--effects of bee stings. - A while back I spent half the day detailing my airplane. I got a thousand dead bugs off the windscreen and leading edges and opened all the doors to give the inside a real thorough cleaning and airing out. As a reward for all my labors, I flew off over the Everglades to practice some maneuvers—and cover the wings with another coat of dead bugs." Full Story: AOPA Online
02/01/2025 Pilot Minute: What is the FAA Researching in Human Factors? - In this new episode of the Pilot Minute video series, Federal Air Surgeon Dr. Susan Northrup provides examples of spatial disorientation and how the FAA is partnering with institutes and institutions to investigate causal factors and how to prevent them. To watch this and other videos, visit bit.ly/FAAPilotMinute.
Also read the Safety Briefing’s “It’s a Confusing World Up There” (medium.com/faa/its-a-confusing-world-up-there-5070c1e5806b) and “Your Senses in the Shadows” (faasteam.medium.com/your-senses-in-the-shadows-5ed018e015b5) for additional information on spatial disorientation and visual illusions.
01/21/2025 The Three “E” Approach — Educate, Early Intervention, and the Evolution of Standards - FAA Safety Briefing Magazine - By Dr. Susan Northrup, FAA Federal Air Surgeon - "I would like to take the opportunity to outline our 2025 goals in the FAA Office of Aerospace Medicine. Some are concrete and easily measurable; others are aspirational but just as important. Recall from the previous issue that we are concerned about both sudden and subtle incapacitation; we must not only consider you the pilot, but society at large. When we can assure ourselves that the risk is acceptable, then we can issue a medical certificate. My goals include:
- In support of the Air Traffic Organization’s air traffic control specialist (ATCS) hiring goal to reduce the shortage, medically certificate at least 2,500 ATCS applicants for the FAA Academy. (This is almost double what we cleared just a few years ago.)
- Fill 95% of all medical officer vacancies to reduce the amount of time necessary to medically certify ATCS candidates and pilot applicants. (Not only have we seen an increase in ATCS applications, but the number of pilot applicants and the complexity of their medical histories have also increased dramatically. We are also seeking to increase the number of aviation medical examiners (AMEs) available for pilot medical certification.)
- Increase the number of behavioral health specialists on... Continue Here.
 |
|
|
The AME Minute is presented by FAA Aviation Safety's Aerospace Medical Education Division of the Civil Aerospace Medical Institute, in association with FAA Media Solutions.
12/16/2024 New Medical Denials Raise Concerns - From AVweb -"The FAA says a new policy on medical deferrals and denials isn’t necessarily permanently disqualifying for Sport Pilot and BasicMed privileges. - The FAA says those who have their medicals denied under a new deferral processing policy will not necessarily be disqualified from obtaining medical certification through BasicMed. Effective Jan.1, anyone whose medical deferral is not accompanied by all the necessary paperwork and reports will have their medical denied. A medical denial makes a pilot ineligible for BasicMed and Sport Pilot. But under the new policy, affected pilots will be able to apply for reconsideration of the denial and if that's approved they will again be eligible for BasicMed and Sport Pilot. Here's the FAA's statement:" Read More Here.
12/11/2024 OK, So Now What? - Part one - From AOPA - "It seems that I stirred up a little bit of a hornet’s nest with the post last month and all those dire statistics. Much of the feedback I got agreed with my reaction of finding those stats pretty shocking, but then the trend was, “I watch what I eat, but I’m still overweight, what’s up with that?” - "The other responses were, “Yeah, that’s pretty bad, OK, so now what?” These issues of diet, obesity, and processed foods causing health problems are hugely complex. To get to the answers, let’s do what we pilots naturally do and pull back on the stick, gain some altitude, and look at the big picture. This month I’ll talk about genetic and metabolic factors that lead to obesity and next month we’ll tackle how it can be managed, in addition to the dietary changes I’ve already stressed.
There’s ample data that supports the principles detailed last month that a significant proportion of the country’s obesity problem is related to choices with diets and lifestyle. Since human genetics haven’t changed and the rate of obesity in America has nearly tripled since the 1960s (70% of our population is now overweight), a lot of this has to be related to environmental factors and life choices. Still, it’s way too simplistic to just write off obesity like a math equation, “take in more calories than you burn and you store all the extra as fat.” To get an idea of just how complex this subject is, click on the National Library of Medicine site, affectionately known as “PubMed“ in the medical world, and type “obesity” in the search bar. You’ll get 48,879 links to recent peer-reviewed medical publications on the topic." Continue Reading Here.
12/06/2024 Microlearning for Aviation Medical Examiners - FAA - AME MOMENT VIDEO - In this microlearning lesson, Dr. Warren Silberman, DO, MPH explains how requirements for testing the Aviation English Language Standard (AESL) differ from medical certification requirements and the importance of obtaining a complete medical history. (Running time: 1:19) - View the presentation Here.
12/06/2024 Federal Air Surgeon's Bulletin -
Pregnancy and FlightBy Susan Buriak DH.Ed, MPH, Susan Jay, Ph.D., MPH and Kyle Copeland Ph.D.The fact that women are in aviation is not a recent phenomenon. Women entered military aviation eighty years ago and were flying aerostats a century before the airplane was invented.1 As more women enter aerospace, it is necessary to address the issue of pregnancy and flight. Pregnancy is a normal physiologic event. Pregnancy is not a disease or an illness. Under normal circumstances, it is not disqualifying for a medical certificate. The FAA recommends that pregnant pilots make their obstetrician aware of all aviation activities they plan to participate in, especially during the third trimester.2 There are several health concerns applicable to the physiology of pregnant aviators:
Hypoxia In a collaborative effort with the Aircraft Owners and Pilots Association (AOPA), the Civil Aerospace Medical Institute (CAMI) has provided information on pregnancy and aviation: per 14 C.F.R. § 91.211, pilots are required to use supplemental oxygen for flights above 12,500 feet up to 14,000 feet, and longer than 30 minutes in duration. Aside from this requirement, the aerospace physiology community typically considers sea level to 10,000 feet to be the physiological “compensatory zone."3 At these moderate altitudes, the healthy body is remarkably capable of compensating for the slightly lower partial pressure of oxygen so the exposure should be uneventful. However, there can be considerable differences in individual tolerance to hypoxia, and several factors such as dehydration and fatigue can negatively impact hypoxia tolerance. The normal blood oxygen saturation level (SpO2) at an airliner's cabin pressure altitude of approximately 8,000 feet is typically between 90 and 93 percent. The body uses a combination of increased depth and rate of breathing, elevated heart rate, and increased cardiac output to make up for the lower partial pressure of oxygen at this cabin pressure altitude. These compensatory mechanisms increase the amount of oxygen that reaches the tissues. Additionally, elevated fetal hematocrit and increased fetal hemoglobin's capacity to carry oxygen ensures that fetal oxygen saturation levels do not decrease very much at these moderate altitudes. In fact, there is a wealth of research data from flight attendants, air medical professionals, and women living at high altitudes concurring that there is minimal proof linking long-term exposure to lower partial pressures of oxygen, either living at 10,170 feet (3,100 meters) or in commercial aircraft, to serious pregnancy-related issues.3 However, a pregnant pilot should be aware of her own unique hypoxia signs and symptoms (via hypoxia awareness training) and be ready to use supplemental oxygen and descend the aircraft if necessary. Fetal Adaptation The oxygen-hemoglobin dissociation curve is a graphical representation that shows the relationship between the partial pressure of oxygen (PO₂) and hemoglobin saturation. At sea level, maternal arterial oxygen saturation follows the standard sigmoid shape of this curve, where an increase in PO₂ leads to greater hemoglobin saturation up to a plateau. Fetal hemoglobin (HbF), which is distinct from adult hemoglobin (HbA), has a dissociation curve that is shifted to the left compared to maternal hemoglobin, and the hemoglobin concentration is approximately 50% greater than maternal hemoglobin.4 This shift reflects fetal hemoglobin’s higher affinity for oxygen,5 allowing the fetus to extract more oxygen from the maternal blood supply. At sea level, this leftward shift enables fetal hemoglobin to achieve 20 to 30% greater oxygen saturation6 than maternal hemoglobin at the same PO₂. At altitude, this leftward shift in fetal hemoglobin’s affinity for oxygen provides a physiological advantage in oxygen delivery and protection against hypoxic stress (subtle symptoms). At 10,000 feet (corresponding to the low end of the physiological compensatory zone; Figure 1), both maternal and fetal hemoglobin O2 saturation is approximately 87-88%, but fetal hemoglobin can maintain this blood saturation level at a lower PO2 compared to adult (i.e., maternal) hemoglobin – an advantage that persists with decreased PO2 (i.e., increased altitude).
Figure 1: Oxygen disassociation curves for human maternal (HbA) and fetal blood (HbF) at constant pH and temperature showing fetal affinity for oxygen at altitude (10,000 ft). (Data from Metcalf J, Bartels H, Moll W. Gas exchange in the pregnant uterus. Phys Rev. 1967; 47(4):789.doi:10.1152/physrev.1967.47.4.782.) While both maternal and fetal PO₂ levels decrease due to lower atmospheric oxygen, maternal arterial oxygen saturation can fall significantly, causing a rightward shift in the oxygen dissociation curve, which corresponds to a decreased affinity for oxygen. This rightward shift is partially driven by the Bohr Effect, where an increase in carbon dioxide (CO₂) and a decrease in blood pH creates acidic conditions, lowering maternal hemoglobin's oxygen affinity and facilitating oxygen release to the tissues and fetus. In contrast, the fetal oxygen dissociation curve retains its leftward shift even at altitude -- as fetal CO2 diffuses into the maternal placenta it creates a more alkaline fetal blood, which in turn increases fetal hemoglobin’s affinity for oxygen.6 The Bohr Effect underlies the differential oxygen affinity of maternal and fetal hemoglobin. In maternal circulation, oxygen is unloaded to the tissues and to the placental circulation to the benefit of the fetus. Meanwhile, fetal hemoglobin's reduced sensitivity to the Bohr Effect maintains its high oxygen affinity, ensuring efficient oxygen uptake.5 The Bohr shift in one direction for maternal blood and in the other direction for fetal blood has been described as the double Bohr Effect .4 This difference ensures that fetal hemoglobin can still bind oxygen more effectively than maternal hemoglobin under hypoxic conditions, thereby preventing fetal tachycardia or bradycardia that could result from reduced oxygen supply.6 By understanding these physiological adaptations, we can better appreciate the mechanisms that ensure fetal well-being during maternal exposure to hypoxic environments, such as unpressurized or high-altitude flight. The in utero human fetus has been compared with a high-altitude dweller, or the resiliency of an adult mountain climber on the Mt. Everest summit.5 These mechanisms underscore the remarkable efficiency of fetal oxygenation strategies to maximize oxygen capacity and optimize oxygen release where it is most needed. Hypotension and G Forces Based on a thorough literature review and analysis of over seven metrics (behavior, body composition, anthropometry, biomechanics, physiology, health and learning), the United States Air Force Academy determined that there are no significant differences in G tolerance between males and females under gradual or rapid acceleration profiles. All factors considered, a woman’s G tolerance was reported to be equal to a man’s.7,8 However, dehydration and low blood pressure caused by hormonal influences on blood vessels are typical during pregnancy. Some abnormal flight conditions such as wind shear, wake turbulence, upset recovery procedures, engine loss, rapid depressurization, and other crises can lead to higher G-loads affecting a pregnant pilot.8 During pregnancy, about 25% of blood flow goes to the placenta and uterus. This lowers systemic blood pressure, raising the risk of syncope and lowering G tolerance .9 Size of Abdomen According to the American College of Obstetricians and Gynecologists (ACOG), pregnant women should wear seatbelts properly adjusted for their safety. The seatbelt should be “positioned low across the hips, between the protuberant abdomen and the pelvis.” 10 When a pregnancy progresses and the uterus grows, the width of the abdomen may impede use of some of the flight controls and interfere with emergency exit maneuvers. Pregnancy and Medication Nausea and vomiting are common during pregnancy, primarily during the first trimester. The only FDA approved medication is docylamine/pyridoxine (Diclegis). The FAA is updating medication guidance for the administration of antiemetic medication for pilots with morning sickness/nausea. When completed this guidance will be available online in the Guide for Aviation Medical Examiners. Medications for conditions that may arise due to pregnancy, such as gestational diabetes, gestational hypertension, postpartum hypertension, and postpartum depression, will follow the existing disposition protocols within the FAA’s medical certification process. These protocols may include issuance by an Aviation Medical Examiner (AME) or deferral to the FAA for a special issuance, depending on the duration of use and the severity of the condition. Circadian Rhythm A brief from the International Association of Airline Pilots’ Association (IFALPA) reported that a pregnant woman needs more sleep than normal due to the associated hormonal and physical changes of pregnancy. Pregnancy-related hormones (progesterone, estrogen, cortisol, and oxytocin) have a significant impact on sleep quality during the third trimester. Research indicates that sleep disorders affect two-thirds of pregnant women. Common sleep disorders include insomnia, nocturnal gastroesophageal reflux, sleep apnea, and nighttime urination. Lack of sleep during pregnancy is linked to pro-inflammatory serum cytokines, which in turn are linked to preterm labor and postpartum depression, longer labor, and a higher rate of cesarean sections. A major factor in chronic sleep deprivation is the disruption of circadian rhythms caused by irregular airline schedules. Pilot performance may be impacted by sleep deprivation brought on by shift work, which has been connected to a higher rate of miscarriages.10 Deep Vein Thrombosis (DVT)/ Pulmonary Embolism A medical history of DVT, maternal age greater than thirty-five years, or a heredity predisposition to DVT are significant risk factors for pregnant women making them 5 times more likely to develop DVT when pregnant (NIH). Other risk factors include previous history of lupus, inherited or acquired thrombophilias, a previous history of thrombosis, antiphospholipid syndrome, heart disease, and sickle cell disease.11 Increased estrogen levels increase blood coagulation. Deep vein thrombosis and pulmonary embolism are among the most common serious vascular diseases that occur during pregnancy. They account for the highest number of obstetric deaths related to blood pressure disorders including hemorrhage and sepsis .” 9 Sitting for prolonged periods of time increases the risk of lower extremity edema, thrombophlebitis, and deep vein thrombosis. According to IFALPA, pilots, and especially pregnant pilots, should walk around every 1 – 2 hours. Other conditions that alter blood flow or normal clotting mechanisms may make some people more likely to develop a DVT. Some of these risk factors include a prior DVT, certain heart diseases, cancer, pregnancy, smoking, older age, and some blood clotting disorders.13 Other blood disorders such as a recent history of thrombocytopenia (within 5 years) due to pregnancy which has resolved, may be issued a regular medical certificate by the Aviation Medical Examiner. A special issuance is not required.14 DVT Risk Mitigation Risks for pregnant aviators are similar to overall risks for passengers and frequent flyers. These include dehydration from lower humidity, as well as edema and DVT due to long periods of immobilization in the flight deck, and edema. ACOG recommends preventive measures including support socks, occasional ambulation and hydration.10 Cosmic Radiation If a pilot is pregnant or considering pregnancy, exposure to ionizing radiation at altitude is a consideration. Cosmic radiation may lead to miscarriage for pregnant aviators. A National Institute for Occupational Safety and Health (NIOSH) study in 2009 reported that exposure to 0.36 mSv (1 milli sievert is equal to 1/1000th of a sievert) or more of cosmic radiation in the first trimester is linked to higher risk of miscarriage.18 Radiation sensitivity of the fetus varies throughout development. According to the International Commission on Radiation Protection (ICRP) the fetus should be afforded the same degree of protection from occupational exposure as members of the public. Therefore, radiation exposure to a fetus should not generally exceed 1 mSv. For cosmic radiation, a pregnant woman’s body does not provide much shielding, so in a practical sense this limit must also be applied to the crewmember to protect the fetus. According to IFALPA, the average annual exposure for a pilot is between 2-5 mSv. Thus, in operational terms, a dose of 1 mSv could be accumulated in significantly less than 9 months of flying. FAA recommends pregnant aircrew limit ionizing radiation exposure to no more than 0.5 mSv per month.16 This limit may be exceeded after only 80 airborne hours on some long, high altitude flight routes.17 The specific number of hours one can fly and keep exposures below these limits depends primarily on route choices and cruise altitudes (flight-dose tools such as FAA’s CARI software and NASA’s NAIRAS website are freely available to the public).
Flight dose calculating software and more information on in-flight radiation exposure is available from the FAA’s Radiobiology Services Website Radiobiology Services | Federal Aviation Administration. Highly unpredictable, solar particle events also occasionally result in significant doses. Solar particle events can be tracked, and there are some advisory messaging systems (International Civil Aviation Organization, national Oceanic and Atmospheric Administration, FAA)18; however, the ability to forecast these events is very limited and not adequate for predicting route dose estimates. The best accuracy for route dose estimation for a flight that occurred during an event requires post-event analysis of all available data. Both solar cosmic radiation and galactic cosmic radiation are deflected and shielded in the same way, so the same factors control (i.e., reduce) exposure: time, altitude, and latitude. Pregnant pilots are encouraged to reduce long flights, high altitudes, and flights over the poles. Returning to Flying Assuming that there are no perineal or other complications, postpartum pilots can return to flying when released by their obstetricians, usually following the traditional six-week recovery period.
Dr. Buriak is an Instructional Program Manager in the Aerospace Medical Education Division at CAMI (AAM-400) Dr. Jay is an Aerospace Physiologist and Team Lead for the Aerospace and Environmental Physiology Research Team at CAMI (AAM-631) Dr. Copeland is a Heath Physicist and Team Lead of the Health Safety Information Team at CAMI (AAM-631) References:1. Davis J, Stepanak J, Fogarty J, Blue R. Fundamentals of Aerospace Medicine. 5th ed. Wolters Kluwer; 2021.2. Guide for Aviation Medical Examiners Item 48. Federal Aviation Administration. Accessed September 22, 2024. https://www.faa.gov/ame_guide/app_process/exam_tech/item48/amd/pregnancy3. Wright B. Altitude and pregnancy. www.aopa.org. Published December 17, 2019. https://www.aopa.org/news-and-media/all-news/2020/january/flight-training-magazine/ol-altitude-and-pregnancy4. Guyton, AC, Hall JE. 11th ed. Textbook of Medical Physiology. Elsevier Saunders; 2006.5. West JB, Schoene, RB, Luks, AM, Milledge JS. 5th ed. High Altitude Medicine and Physiology. CRC Press; 2013.6. Davis, JR, Johnson R, Stepanek J, Fogarty JA. Fundamentals of Aerospace Medicine. 4th ed. Lippincott Williams & Wilkins; 2008.7. Waterman KM and Miller JC. Women in Military Aviation. United States Air Force Academy, Colorado Springs CO May 2000 USAFA TR 2000-06.8. Gillingham KK, Schade CM, Jackson WG, Gilstrap LC. Women’s G Tolerance. Aviation, Space, and Environmental Medicine, 1986;58(8): 745-753.9. International Federation of Air Line Pilot’s Associations (IFALPA). Pregnancy and Flying: Human Performance Briefing Leaflet 18HUPBL02. London, UK; 2018.10. American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 746 Summary. Obstet & Gynecol. 2018;132(2):533-534. doi: 10.1097/aog.0000000000002758.11. Devis P, Knuttinen MG. Deep venous thrombosis in pregnancy: incidence, pathogenesis and endovascular management. Cardiovasc Diagn Ther. 2017;7 (Suppl 3):S309-S319. doi:10.21037/cdt.2017.10.08.12. Shennan AH, Green M, Ridout AE. Accurate surveillance of maternal deaths is an international priority. BMJ. 2022; 379. doi:10.1136/bmj.o2691 PMID: 36384947.13. Federal Aviation Administration (FAA). Deep Vein Thrombosis. Aeromedical brochure. https://www.faa.gov/sites/faa.gov/files/pilots/safety/pilotsafetybrochures/DVT.pdf.
|

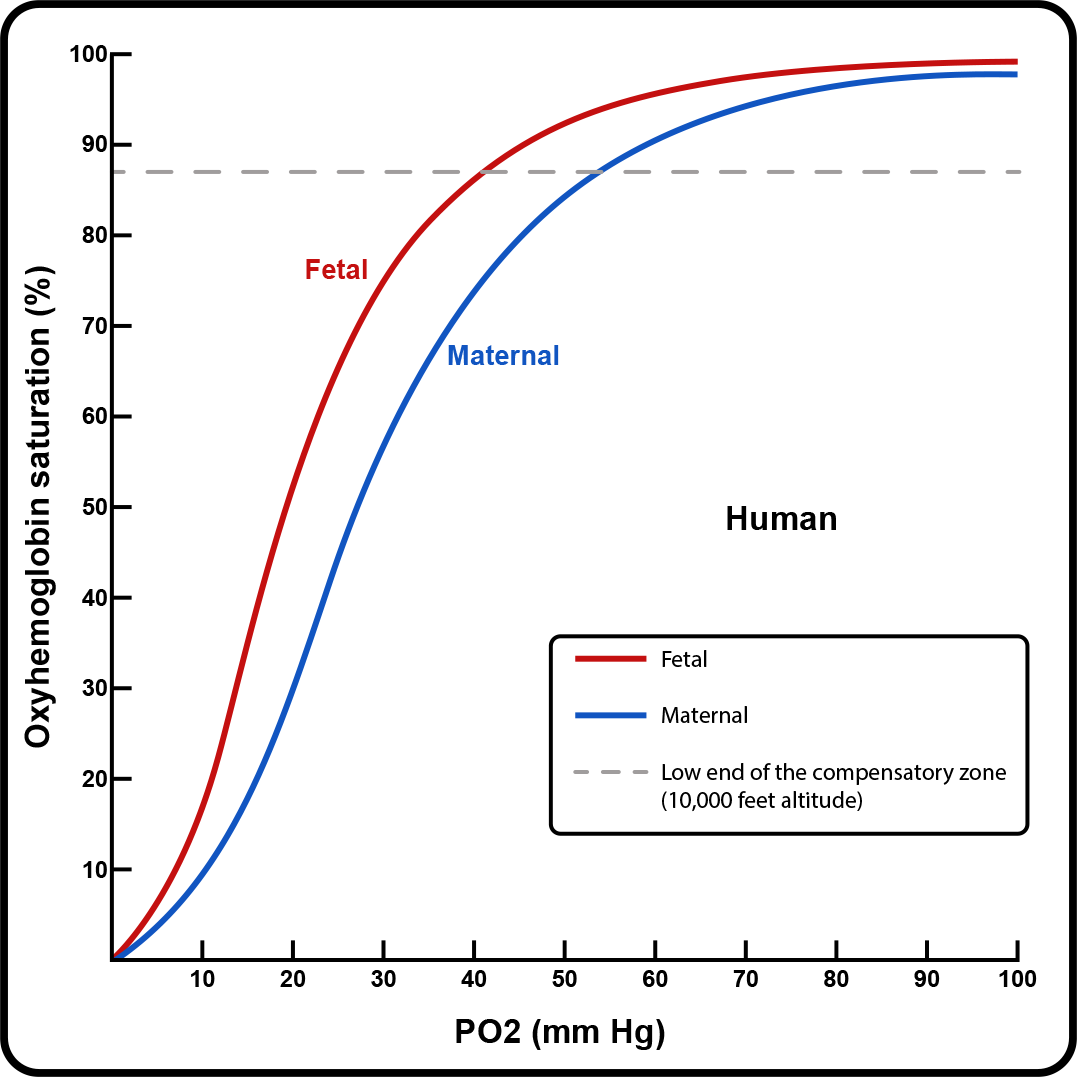
|
|
Spatial Disorientation
By Jason Sigmon MD, FACS
Spatial Disorientation represents a hazard to aviation safety when it leads to a failure by the aviator or flight crew to sense correctly the position, motion, or attitude of the aircraft or of him/herself within space in relation to the earth. While failure of cockpit instrumentation and erroneous information can precipitate these accidents the factors involved are primarily human ones.
Spatial disorientation has been a recognized hazard since the dawn of human flight and to this day represents an area of robust research into its complex nature. It was understood very early in human flight that pilot’s had difficulty maintaining safe orientation of an aircraft in the absence of a visible horizon. Advances in awareness and aircraft instrumentation, such as the Sperry artificial horizon, allowed for safer pilot operations and fewer spatial disorientation accidents.
While the artificial horizon was a key development in advancing the capability of aircraft operations spatial disorientation accidents continued to be a significant aviation safety concern accounting for approximately 16-20% of all fatal accidents. This led our aerospace physiology and medicine colleagues to seek out a better understanding of the human sensory system and its role in errors of orientation when piloting an aircraft. We now have a better understanding of the combined contribution of the visual and vestibular systems and the factors in flight that lead to inaccurate pilot interpretation of sensory cues.
While the incidence of aircraft accidents secondary to spatial disorientation has decreased steadily over the years, the problem persists. Our most recent spatial disorientation study at CAMI shows that approximately 10% of Part 91 general aviation fixed wing accidents between 2003 and 2021 involved spatial disorientation as the primary cause after NTSB final evaluation. As has previously been reported in prior studies over 90% of these accidents unfortunately are fatal to the pilot, passengers or even individuals on the ground.
The office of aerospace medicine is addressing the hazard of spatial disorientation in the following ways:
I. Aerospace Medical Certification
While any human engaged in piloting in aircraft in environmental conditions of diminished visibility is at-risk for spatial disorientation, it is important that the medical evaluation of pilots with potential underlying acute or chronic conditions of the inner ear or vision are identified and managed effectively to ensure aviation safety.
In 2023, the office of aerospace medicine updated the AME guide with aerospace medical disposition tables for the following conditions affecting the inner ear:
- Acoustic Neuroma
- Benign Paroxysmal Positional Vertigo
- Labyrinthitis
- Meniere’s Disease
- Motion Sickness
- Perilymph Fistula
- Persistent Postural Perceptual Dizziness
- Superior Semicircular Canal Dehiscence Syndrome
II. Human Factors Research
The human factors research division at CAMI continues to study potentially contributing factors to spatial disorientation accidents including the global cognitive impact of fatigue as well as the specific performance impairment of medications or substances.
A new retrospective accident study conducted by CAMI’s Human Factor’s Research Division evaluated the incidence of positive post-mortem toxicology for potentially impairing medications and substances in general aviation spatial disorientation fatalities. Approximately one-third of the accidents in the study included a positive toxicology finding from CAMI’s toxicology laboratory.
Future areas of research in spatial disorientation include a need to better understand how pilot’s cognitively prioritize tasks when operating their aircraft in diminished visual conditions or while performing maneuvers conducive to spatial disorientation. Many spatial disorientation accidents include errors in decision-making and the inadequate use of available weather information. Research focused on a better understanding of how a pilot utilizes and processes information when making decisions is another example of the increased focus on cognition in the field of spatial disorientation research.
III. Airman Education
Ample evidence supports the positive impact of pilot training and experience in the prevention and mitigation of spatial disorientation accidents.
At CAMI, our Airman Education program is developing a comprehensive spatial disorientation practical training program for pilots utilizing our two GATS-II full motion aircraft simulators and airman education physiology team.
This full-day course includes didactic classroom presentations on the topics of inner ear and visual physiology, SD accident case-studies, fatigue and the impact of potentially impairing medications or substances. The practical element of this course includes pilot participation in operationally relevant spatial disorientation flight scenarios utilizing the GATS-II full motion simulator(s).
Dr. Sigmon is a Medical Officer and Regional Flight Surgeon (International/Military/Federal) in the Aerospace Medical Education Division at CAMI (AAM-400)
|
|
Medical Certification Policy Updates
By Judith Frazier, MD, MBA
The Policy and Standards branch continues to focus on helping Aviation Medical Examiners (AMEs) more easily obtain the information needed to make a medical certification decision. This version highlights policy changes and updates published between June 2024 and October 2024. The full list of changes is hyperlinked in the Archives and Updates section of the AME Guide.
Psychiatry/Behavioral Health
Anxiety, Depression and Related Conditions– updated to remind AMEs to list/identify in block 60 which diagnosis are being use for Fast Track. Added single page with all the conditions/diagnosis which can be used for this program.
Attention-Deficit/Hyperactivity Disorder (ADHD) Disposition Table
- Clarified it is applicable for both pilots and ATCS
- Can accept if meets both Fast Track for ADHD AND Fast Track for Anxiety Depression and related conditions,
- Standard Track, clarify that separate tests must be ordered for BOTH amphetamines AND methylphenidate.
FAST TRACK PATHWAY Decision Tool for Current Deferred Cases for depression, anxiety, and related conditions available for AME use. Combines all required items for Fast Track in one place.
Neurology
CACI – Migraine and Chronic Headache Worksheet – revised to add additional medications.
Head Injury or Brain Injury Disposition Table – expanded guidance for brain injury 5 or more years ago (Row B1) or brain injury within the past 5 years (Row B2).
Brain Injury Decision Tool for the AME – new to use with Brain Injury dispo table.
Neurology – Section updated grouping all items attached to a condition in a single place (dispo table, CACI, AASI, status summary). Align entire section as a single search page.
Otolaryngology (ENT)
ENT – New Disposition tables for:
- Allergies or Anaphylaxis; (Allergic Rhinitis; Seasonal Allergic Rhinitis; Hay fever) Disposition Table.
- Sinus Conditions Dispositions Table.
- Speech Impediment - Stuttering, or Mechanical Conditions Disposition Table
Other Systems
Cardiology – ECG/EKG - AME Equipment and Medical Confidentiality, EKG/ECG equipment must be 12-lead.
Dermatology (Skin) – New Psoriasis Disposition Table, CACI – Psoriasis Worksheet and AASI – Psoriasis. Updated meds allowed for CACI
GI – CACI - Colitis Worksheet revised to add additional acceptable medications.
GU – Low Testosterone (Low T) Hypogonadism New Disposition Table, new CACI, new AASI, new Status Summary.
ID – Updated COVID-19 disposition table. AMEs no longer required to annotate uncomplicated, resolved COVID infection.
Musculoskeletal – Pectus Excavatum Disposition Table. (new)
Arthritis CACI – expanded to add additional medications.
Rheumatology – CACI - Arthritis Worksheet revised to add additional acceptable medications.
Miscellaneous
New page added for English Proficiency and Pilot Medical Certification. English language is not a medical requirement. Described what an AME should look for and if concerns, can opt to report to the FSDO.
Terminology update. Aviation psychiatrist or Aviation psychologist replaces term HIMS psychiatrist or HIMS psychologist.
Exam techniques – revised Item 35 Lungs and Chest; Item 39. Anus, Examination Techniques revised, and Item 41. G-U System, Examination Techniques
Updates. Describes what part of exam is not required unless indicated by past medical history or symptoms. It may be performed at the discretion of the AME or applicant. Document findings in Item 60.
Pharmaceuticals
Pharmaceuticals – Weight Loss Management Medications and Pre-Diabetes. Expanded the acceptable meds for CACI to include tirzepatide (GIP + GLP-1 Agonist) Mounjaro or Zepbound
Biologics, Biosimilars, and Non-biologics – new page Expands acceptable medications for colitis, psoriasis, and arthritis.
Migraine Medication – new page. Expands acceptable medications including for CACI.
Over-the-Counter Medications Reference Guide (What Medications Can I Take and Still Be Safe to Fly) – added to AME guide
Vaccines – reduced required observation time after COVID vaccine to 24 hours if no symptoms.
Administrative Changes
Special Issuances – removed AASI Certificate Issuance Coversheet. This document is no longer needed.
Help us improve the AME guide! Send you comments or suggestions to: AMEGuide@FAA.gov. (This mailbox does not answer case questions.)
Dr. Frazier is the Manager of the Policy and Standards Branch in the Office of Aerospace Medicine (AAM-220).
|
11/27/2024 How Business Aviation Pilots Are Staying Safe and Alert - "Piloting aircraft for long periods of time not only reduces concentration and reaction time – it can contribute to deadly accidents. If your business aviation operation doesn’t have a fatigue mitigation program, maybe it should. - Long-range aviation has leaped lightyears ahead in the century since “Lucky Lindy” completed his 33-hour solo slog from New York to Paris. With their super-efficient engines, GPS-based navigation and satellite-based connectivity, today’s ultra-long-range business jets can easily leapfrog the globe. - However, those aircraft capabilities still have to accommodate crew member flight fatigue. Sitting for hours, even in the most comfortable seat, can take a considerable toll on a pilot’s alertness. So why don’t flight departments pay more attention to the dangers of fatigue? - “The majority of long-distance business aviation flights aren’t..." Finish Reading Here.
11/27/2024 AIr Sickness: A Pilots Guide to AI-Powered Health - "On August 4, 1997, the United States Congress passed a funding bill; a mere 25 days later the implications of that act became apparent, and those in power realized they had made a dreadful mistake havinginitiated an existential disaster for humanity. - The referenced legislation was, of course, to empower Skynet to manage the North American Aerospace Defense Command, removing humans from decision-making. Skynet became self-aware and, recognizing humans were the single biggest threat to humans, launched a preemptive nuclear strike on Russia leading to global devastation.
For those not familiar, the above scenario was the basis for the Terminator series of movies and inspired widespread fear of artificial intelligence, AI. As computing became more widespread there were always those to present the downside or prophesize doom, from the now-famous IBM president who in 1943 said, “I think there is a world..." Read the treatise Here.
11/15/2024 BasicMed expansion - Federal law recognizes the safety of the program by and for GA pilots - From AOPA - "The expansion of BasicMed privileges included in the 2024 FAA Reauthorization Act of 2024 is now in full effect as of November 12. - Under the new law signed May 16, pilots may now use BasicMed privileges to fly aircraft weighing up to 12,500 pounds and certified to carry up to seven occupants. The previous aircraft weight limitation was 6,000 pounds, with certification for up to six occupants. - Full Story Here.
11/07/2024 AME Minute: Why did the FAA develop a new CACI for Low T? - VIDEO - In this microlearning lesson, Dr. Warren Silberman, DO, MPH lists medications for hypogonadism which are now accepted for medical issuance under the CACI program and the required criteria and documentation. - Watch Here
10/26/2024 Federal Air Surgeon Addresses Mental Health Progress, Deferral Delays - "Federal Flight Surgeon Dr. Susan Northrup, center, gave an update on mental health initiatives at the FAA. - Federal Air Surgeon Dr. Susan Northrup says a pilot medical Bill of Rights is under development, a shorter time lag for pilots to regain their privileges after a medication change is on the way and sometime in the future there will be a "period of non-enforcement" to allow those with undeclared history or challenges with mental health to get the help they need without fear of sanctions. During a Q and A at the National Safety Forum at NBAA-BACE in Las Vegas on Wednesday, she also said the backlog delay of medical deferral decisions has been reduced from a year to less than three months and will be reduced further. She's also hoping that those awaiting their deferrals will soon be able to accurately track their progress accurately online in real time.
Northrup was in Las Vegas to specifically address mental health issues in aviation, notably the well-known practice of lying about mental health problems to avoid deferrals and..." Full Story Here.
10/09/2024 We're Not Aging Well - From AOPA - "A lot of people, including Colin Powell who made the phrase popular, have observed that bad news isn’t like good wine – it doesn’t get better with age. Unfortunately, the same can be said for progressive generations of young Americans whose bad news is that over the decades they aren’t aging well either. - While doing some background reading for the last few articles on health, diet, and energy drinks, I kept coming across more and more information on just how unhealthy we’ve become in this country. I mentioned last month that processed foods were leading to earlier and more deadly colon cancer in young people (<50 years old) due to poisoning and premature aging (senescence) of the cells lining the GI tract that render them unable to fight off tumor formation. Increasing cancer rates in younger generations is not unique to just GI cancer; it turns out that every generation of Americans has a progressively higher rate of lots of different types of cancer than the preceding generation. An article published just this month in The Lancet with..." Read the whole article Here.
10/01/2024 FAA Reduces Mandatory COVID-19 Vaccine Pilot Wait Time - "The agency's updated Guide for Aviation Medical Examiners says the wait time has been cut from 48 hours to 24 hours, provided the pilot doesn't show symptoms after 24 hours." More Here.
09/18/2024 VIDEO: Leukemia and Lymphoma - Can I get a medical certificate if I have a history of leukemia or lymphoma? - In this recent episode of the Pilot Minute video series, Federal Air Surgeon Dr. Susan Northrop describes how AMEs can issue a medical certificate for these conditions and how pilots can expedite the process. - Pilot Minute Video Here.
09/06/2024 VIDEO: Why should I be concerned about herbal remedies? - In this episode of the Pilot Minute, Federal Air Surgeon Dr. Susan Northrup lists the herbal remedies and supplements that are not acceptable for medical certification, including specific concerns for aviation safety. - See the Video Here.
09/06/2024 AME Minute - FAA - Microlearning for Aviation Medical Examiners - In this microlearning lesson, Dr. Warren Silberman, DO, MPH explains how distinguishing head injuries from brain injuries reduces deferrals to the FAA, and allows AMEs to issue medical certificates under a new option. (Running time: 1:22) - The AME Minute is presented by FAA Aviation Safety's Aerospace Medical Education Division of the Civil Aerospace Medical Institute, in association with FAA Media Solutions. Watch Video Here. - To provide feedback, please email ame-distance-training@faa.gov
08/11/2024 Be careful what you put in your tank - FROM AOPA - "Energy drinks can deliver a boost, but it is important to be aware of their possible side effects." Continue
08/10/2024 Latest Pilot Minute Video Covers Herbal Remedies - FAA - VIDEO - Pilots may wonder, “Why should I be concerned about herbal remedies?” Not all organic substances are safe and some can have similar effects to those of illicit drugs. In the latest episode of the Pilot Minute video series, Federal Air surgeon Dr. Susan Northrop explains the herbal remedies and supplements that are not acceptable for medical certification including specific concerns for aviation safety. Go to youtube.com/watch?v=u1-FIcnqDms&list=PL5vHkqHi51DQvRjGJo1SuXyZpKl5HbzOI to watch this and other Pilot Minute videos.
07/15/2024 From NBAA - The FAA recently issued new guidelines indicating that the agency is changing its criteria for evaluating pilots’ mental wellness, giving medical examiners greater autonomy in evaluations. Listen as a panel of mental-wellness experts takes listeners behind the headlines to discuss ways the changes might impact aviators’ readiness for flight. - In this episode of NBAA’s “Flight Plan,” host Rob Finfrock speaks with:
07/13/2024 Latest Pilot Minute Video Covers Weight Loss Medications - Pilots may wonder, “Can I take a weight loss drug and still fly?” The FAA allows multiple medications for weight loss, including some available over the counter and some categories of prescription diabetic drugs. In the latest episode of the Pilot Minute video series, Federal Air surgeon Dr. Susan Northrop explains how weight loss medication can be approved by your AME. If you have concerns about weight management, talk to your AME and visit the links in the video description. Go to bit.ly/FAAPilotMinute to watch this and other Pilot Minute videos.
07/09/2024 Microlearning for Aviation Medical Examiners - VIDEO - FAA - In this microlearning lesson, Dr. Warren Silberman, DO, MPH answers a question posed during a recent Grand Rounds session regarding online access to most recent and historical medical certification policy updates. (Running time: 57 seconds) - View it Here. - The AME Minute is presented by FAA Aviation Safety's Aerospace Medical Education Division of the Civil Aerospace Medical Institute, in association with FAA Media Solutions.
6/30/2024 Aeromedical Summit, an ARC, and Grand Rounds - By Susan Northrup, MD, MPH - Federal Air Surgeon - Welcome to the June 2024 Federal Air Surgeon’s Medical Bulletin! A LOT has happened in the last six months. My thanks to each of you for taking this journey with us as we update the medical standards and IT infrastructure. I appreciate your patience as we introduced double authentication for AMEs accessing our medical subsystems. For most people, it was seamless, but not for all. You can expect further enhancements and improvements in our system moving forward.
The Mental Health and Medical Clearance Aviation Rulemaking Committee (ARC). In December 2023, the FAA Administrator announced the formation of the ARC to evaluate the barriers to pilots seeking mental health support and treatment and reporting it to the FAA. The ARC was made up of people from industry, academia, pilot advocacy groups, unions, peer support organizations, flight training organizations, and aerospace medicine mental health experts. Observers and subject matter experts included international partners, representatives from the NTSB and FAA, and other interested parties. In less than four months from inception, the ARC produced a report discussing the barriers and providing 24 recommendations. The Office of Aerospace Medicine did not wait for the final report to begin implementing new ideas and accelerating efforts already in progress. As a result, we approved three new medications (SNRIs) in April and updated mental health policy in May to allow AMEs to issue Certificates to more pilots and air traffic controllers who meet certain criteria. For more information see Item 47. Psychiatric Conditions in the AME Guide.
To that end, we continue to encourage everyone to help spread mental health awareness to the entire aviation community. Our efforts have three main themes. I call them the 3-Es.
- Educate all people in the aviation community to reduce stigma and fear regarding FAA processes and policy.
- Early Intervention is key through education, peer support networks, outreach, and if required treatment.
- Evolve medical standards as new science develops.
One of the outcomes from both our Aeromedical Certification Summit and the ARC was a recommendation to provide AMEs more frequent training and education, particularly when we make major changes in policy. In May, we stood up Grand Rounds -- notifications were sent out through AMCS and emails. Approximately 20% of the AMEs attended. The feedback was uniformly positive. And, we provided one hour of CME. Please understand, these sessions are not to discuss specific cases. The design is to provide current policy updates or items generating a lot of interest or questions. We will accept recommendations for future topics.
The Grand Rounds will be scheduled the last week of each month. Information and the virtual meeting link will be send to AMEs via email. - Finally, thank you for all you do to keep the National Air Space safe. - Susan
06/30/2024 - Medical Certification Policy Updates - By Judith Frazier, MD, MBA - The Policy and Standards branch continues to focus on helping Aviation Medical Examiners (AMEs) more easily obtain the information needed to make a medical certification decision. This version highlights policy changes and updates published between November 2023 and May 2024. The full list of changes is hyperlinked in the Archives and Updates section of the AME Guide.
Psychiatry/Behavioral Health - Anxiety, Depression and Related Conditions – introduced new disposition table and a new Decision Tool for the AME. Using this tool, AMEs may be able to issue a combination of up to two (2) behavioral health diagnoses when uncomplicated, treated with a single medication 2 years ago or longer.
If currently in psychotherapy and no medication, may also be issued using the Decision Tool. Remember to put the specific wording from the dispo table in Block 60 so we know you used the Decision Tool!
Expanded acceptable antidepressant medications (previous known as the SSRI protocol) to include EIGHT (8) medications of various classes (SSRI, SNRI, and NDRI).
Post-Traumatic Stress Disorder (PTSD) – revised the disposition table to allow ongoing psychotherapy. - Need to reach an FAA psychiatrist with a question? Use the new Branch email 9-AVS-Psychiatry-Branch@faa.gov.
Cardiac
Coronary Heart Disease (CHD) – Expanded disposition table added listing out initial certification requirements by class. Corresponding Protocol page added.
Recertification. Simplified the AASI for CHD requirements for recertification for all classes by removing the annual stress test. If currently on an AASI for CHD/CAD, the RECERTIFICATION evaluation data is based on control of risk factors. Have the treating cardiologist complete the Coronary Heart Disease (CHD)/ Coronary Artery Disease (CAD) Recertification Status Summary. Please let your pilots know about this new change as we started to update their authorization letters!
If risk factors are not controlled, a stress test may be required. If currently on a SI, the CHD/CAD Recertification Status Summary should also be submitted to expedite recertification along with any stress testing requested per the authorization letter.
Atrial Fibrillation (A-Fib)/A-Flutter – Simplified Status Summary to use for both Initial and Recertification. Rember to send in the clinic notes showing how the A-Fib/Flutter was diagnosed for INITIAL certification consideration.
Chest Pain/Angina – New disposition table.
ECG/EKG – Clarified a full 12-lead ECG is required. (1,2, or 6 leads are not acceptable). Must be 25mm/sec at 10 mV.
Hemoglobin A1c replaces a fasting blood sugar on multiple cardiac pages and protocols.
Pacemaker – Status Summary expands recertification based on Estimated Replacement Interval. Pilots can be issued an annual SI until the month prior to the ERI expiration which is typically 3-4 month of battery life remaining.
Valve repair and Valve replacement – simplified. Removed requirements for stress testing for all classes.
Otolaryngology (ENT)
ENT – Section updated. Expanded and updated disposition tables for both Middle Ear and Outer Ear.
Cochlear implant – new disposition table.
Vertigo – New or expanded disposition tables for vertigo conditions such as Benign Paroxysmal Positional Vertigo (BPPV), Labyrinthitis (Vestibular Neuritis, Viral labyrinthitis, Epidemic Vertigo, Acute Vestibulopathy), Meniere’s Disease, Perilymph Fistula (PLF), Persistent postural Perceptual Dizziness (PPPD or 3PD) and Superior Semicircular Canal Dehiscence Syndrome (SSCDS).
Other Systems/Miscellaneous
GI – Cholelithiasis. Updated disposition table.
Medical Certificate Limitations – Added reference to limitations by system.
Neurology – Syncope. Expanded disposition table. New Chiari Malformation Disposition Table. Added caffeine use to social history the FAA Specifications for Neurologic Evaluation.
Ophthalmology – Lattice Degeneration. New disposition table.
Pharmaceuticals
Pharmaceuticals – Weight Loss Management Medications added as CACI. New Weight Loss Management Status Report (to use with CACI or SI). Clarified Loperamide should not be used for acute illness.
Help us improve the AME guide! Send you comments or suggestions to: AMEGuide@FAA.gov. (This mailbox does not answer case questions.)
- Dr. Frazier is the Manager of the Policy and Standards Branch in the Office of Aerospace Medicine.
6/28/2024 Drug Abatement Program's Latest News - FAA - The Department of Transportation (DOT) published three notices in the Federal Register on June 21, 2024 that pertain to its final rule that authorized employers to use oral fluid drug testing as an alternative testing methodology to urine drug testing. For more information and a link to the DOT’s notices, please visit https://www.transportation.gov/odapc/frpubs. If you have any questions, you may contact the DOT’s Office of Drug and Alcohol Policy and Compliance at 202-366-3784 or ODAPCWebMail@dot.gov.
Remember to visit the FAA’s website at www.faa.gov/go/drugabatement often for updated resources, new or updated FAQs and Q&As, a copy of our latest inspection guide, and other useful materials. Webmaster: Please be aware that at times links to FAA.gov pages sunset and are updated to different locations. Should that become the case, please inform the webmaster at contactus@scauwg.org Thank You!
06/28/2024 FAA Removes Check Pilot Medical Requirement - Rule also eliminates FAA regulatory inconsistencies - The FAA has finalized the substantive relief proposed five years ago that removes a requirement for check pilots, check flight engineers, and flight instructors to Part 135 and 121 operations to hold an FAA medical certificate when performing in-flight duties. This move also eliminates Part 135 and 121 regulatory inconsistencies.
“Removing the conflicting medical certificate requirement enables the utilization of pilots who are otherwise qualified to function as check pilots, check flight engineers, and flight instructors in aircraft,” according to the agency. This relief “would increase the number of experienced pilots who would be able to qualify as Part 135 check pilots on aircraft.” Similar clarifying changes were also made to Part 121. More Here.
06/28/2024 New Pilot Minute Video: How Being Hot and Thirsty Can Affect Flying - In the latest episode of the FAA’s Pilot Minute video series, Federal Air Surgeon Dr. Susan Northrup explains the physiological impacts of dehydration on flying and suggestions for mitigation. See this and past Pilot Minute videos here: https://www.youtube.com/playlist?list=PL5vHkqHi51DQvRjGJo1SuXyZpKl5HbzOI.
06/27/2024 Microlearning for Aviation Medical Examiners - VIDEO - In this microlearning lesson, Dr. Warren Silberman, DO, MPH explains the importance of reviewing ECG lead placements for common errors before uploading to the FAA. (Running time: 1:20) View The Video Here
The original AMEPilot Data is found here:
Welcome to AMEPilot, a new feature of SCAUWG.ORG presented by Aviation Medical Examiner - Gregory J. Hanker, M.D. – Dr. Hanker is an orthopedic surgeon practicing at the Southern California Orthopedic Institute in Van Nuys.

Dr. Hanker’s primary goal as an Aviation Medical Examiner and the author of AMEPilot is to assist the local aviation community in obtaining their medical certification, especially complex cases where FAA special authorization may be necessary.
AMEPilot is a quarterly authored contribution written exclusively for SCAUWG.ORG.
The FIRST EDITION - SPRING - addresses the behind the scenes, rarely known items about how to prepare for and what YOU CAN DO to make your Medical proceed easy and fast! Underlying medical issues can be addressed successfully. When properly prepared and with the proper documentation, only a very small percentage of applications for a medical certificate are denied. Dr. Hanker details how you can mobilize your application for success within the best possible timeframe. The editions that follow continue to provide you with the important data that will help you facilitate your medical application as well as stay in the best possible health and professionally prepare for safe flight.
- NEWSWORTHY NOTE From AOPA: 03/29/2021
Make your selection here:
EXTRA Feature WINTER Dec. 2023 - AOPA- HERE
AMEPilot 2023 SPRING CLICK HERE
AMEPilot 2022 SUMMER CLICK HERE
AMEPilot WINTER 2022 CLICK HERE
AMEPilot 2021 MAY CLICK HERE
AMEPilot 2020 FALL WINTER CLICK HERE
AMEPilot 2020 SPRING SUMMER CLICK HERE
AMEPilot 2020 WINTER EDITION CLICK HERE
AMEPilot 2019 FALL EDITION CLICK HERE
AMEPilot 2019 SUMMER EDITION CLICK HERE
AMEPilot 2019 SPRING EDITION CLICK HERE

Aviation Medical Examiner Gregory J. Hanker, M.D., an orthopedic surgeon practicing at the Southern California Orthopedic Institute in Van Nuys. Tel. (818) 901-6600
Dr. Hanker is a former USAF transport pilot who flew the C-9A Nightingale on aero- medical evacuation missions in Europe; an Ohio USAF Reservist flying the C-123 Provider while attending medical school;
and currently a general aviation pilot flying out of Van Nuys Airport.
Dr. Hanker’s primary goal as an Aviation Medical Examiner (AME) is to assist the local aviation community in obtaining their medical certification, especially complex cases where FAA special authorization may be necessary.